
Rotator Cuff Syndrome, Bursitis or Impingement
All of these describe a painful shoulder and they all mean that the tendons are inflamed.
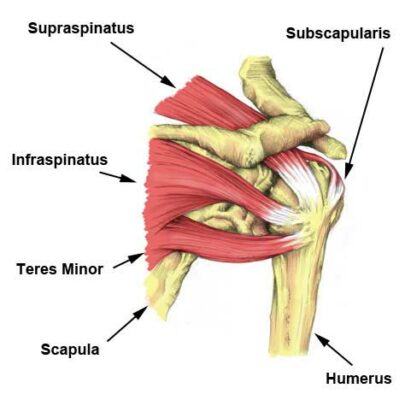
The Rotator Cuff is comprised of 3 tendons of 3 muscles and the main one that causes problems is usually the Supraspinatus.
If you have symptoms of intermittent catching pains on certain movements and you have pain at night especially sleeping on that side, then you may have tendonitis.
The tendons run through a tight space in the shoulder and any inflammation and swelling in the tendon will catch on the bone and lead to pain on movements such as lifting the arm or putting on clothes.
Causes
Often there is no obvious cause but can be from years of poor posture. In other cases it can be from a job or hobby that involves overarm activity repetitively. Other causes can be a fall, tennis golf or overdoing the weights at the gym.

Symptoms
Pain is the first symptom which comes and goes during the day intermittently and it may become worse in the evenings and at night. The pain is often not so severe that you seek treatment until it makes sleeping difficult. The pain usually stays around the shoulder and upper arm but if it goes in to the hand it is more likely from the neck and not the shoulder.
The next step is to see the GP and he will prescribe anti- inflammatories and some physiotherapy. The physiotherapist will advise you what to do, what to avoid and the correct exercises to correct the problem.
If this does not resolve the problem, then you may need to see a shoulder specialist.
The specialist will take down a full history of the condition and examine the shoulder to rule out any other shoulder conditions. If the cause is a tear in the tendon there will have been a significant event such as a big fall to cause this as tendons do not tear easily. The other cause that it can be is “wear and tear” of the tendon which is a chronic problem where the tendon gets rubbed through as you age.
Tests to diagnose Tendonitis?
There are several different types of investigations starting with a good old fashioned Xray. These must be done in the correct way, however, otherwise they do not tell the whole story.
Another very useful investigation for the rotator cuff is an Ultra-sound Scan (USS). This is a dynamic scan during which the radiologist can move your arm around and see what is happening when you move. With a good machine and an experienced radiologist , they can see what is inflamed and the state of the tendon and whether it has a partial or full tear or is just inflamed. They can then inject steroid directly to the area around the inflammation to settle the pain down.
Steroid is a very strong anti-inflammatory medication and is a very effective treatment. However, you should not have too many of them and so it is worth having it done by an expert who directs it to the correct place. It is best not to accept one from your GP but ask to go to a specialist. If you did have one from your GP that did not work it is still worth another try with a specialist with ultrasonic guidance.
Treatment
In about 60% of cases an injection and physiotherapy will cure the problem
If the injection does not give lasting relief then you might need a small operation
The injection
This is usually a mixture of 80mg of Depomedrone (a steroid ) and 8mls of Chirocaine (local anaesthetic ) through the back of the shoulder.
Putting the needle in through the back is the most accurate way of getting into the subacromial space – the gap between the tendon and the bone – and this runs from the back all the way to the front. So an injection placed by this route actually allows the steroid to bathe the whole of the tendon.
After the injection
In some people the shoulder can be a lot more painful for a couple of days. So if you have a long drive or something important in the two days after a proposed injection then it may be worth deferring the injection for a time when you have a few normal days afterwards – just in case.
You can keep taking your normal pain-killers or anti-inflammatories for the next few days. If the injection is going to work you will know and you will feel that there is no pain and then you stop all the tablets.
It is best to rest the shoulder for about 4 – 5 days and try to go to the physiotherapist for a couple of sessions.
The physiotherapist will look at your posture which may have contributed to the problem and they will set about correcting any muscular imbalance in the shoulder. If the pain has settled with the injection this is a good moment to start correcting the problem and building up the rotator cuff muscles and the scapular stabilisers.
Do not rush back to the gym too early to lift heavy weights.
Then ease back in to sport over the next few weeks and may be consider some coaching to correct any faults in your technique that may have contributed to the problem.
Also try to maintain a good sitting posture and continue working at the specific shoulder exercises given to you.
See exercises for Rotator cuff and Scapular on separate sheet.
If the injection done by the shoulder specialist does not cure you for more than a few weeks then it is time to consider surgery. This would normally be a simple decompression which shaves off a little bit of bone to make more space for the tendon.
Sources- extracts take from Mr Sinnerton FRCS Shoulder specialist