

Knee replacement is now the most common type of joint replacement and the number performed each year is rising.
In 2016 a total of 110,000 replacements were performed in the UK which is 30% more than 6 years earlier.
The average age for the procedure is now 69 and the cause is mainly osteoarthritis.
Obesity has been blamed for the increase in demand from the younger patients. Obesity causes an increase in pressure on the joint, which can cause it to wear out faster.
If you have a BMI over 30 you are 4 times as likely to get arthritis and if your BMI is over 40 this raises your risk level to 20 times!
There has been some concern amongst the surgeons that some people are requesting surgery too early. With people living well in to their nineties this may require 2 revisions of knee replacement which will be a more complicated procedure.
The timing of the operation is important delaying as long as possible but before the patient suffers too much muscle loss and ability to walk.
Many doctors will try conservative measures first which will include physiotherapy, exercise, painkillers and encouraging weight loss.
Steroid injections can also be useful in easing pain and inflammation.
Osteotomy
This is sometimes performed to buy time and prevent the need for knee replacement for a further 10-15 years. In this operation bone is added or taken away to shift weight bearing away from the damaged area.This is a good operation to do for those who want to remain active, although recovery time is much the same as for a knee replacement.
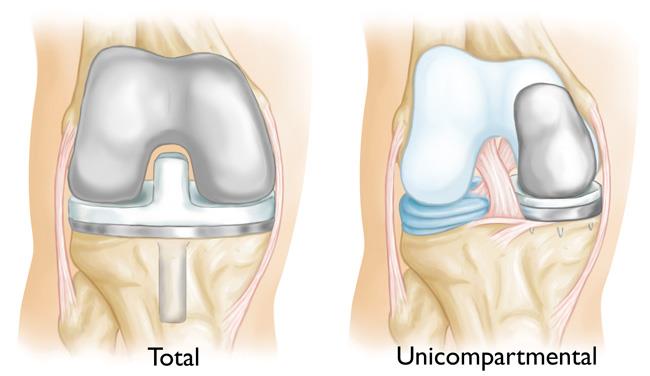
There are 2 types of replacement Full (TKR)and Partial (PKR)
The big advantage of the Partial is that it is a smaller operation, which preserves the ligaments, so it has a higher chance of feeling like a normal knee. The partial replacement makes revision of the surgery at a later date easier.
It is, however, important to choose a surgeon who does a lot of these operations or the outcome may not be as good as having a Total knee replacement.
With total knee replacement some of the ligaments have to be sacrificed usually one or both cruciate ligaments. These are the ligaments that stabilise forward glide and rotation.
After surgery patients have to expect to work hard to get the full function of the knee back with performing regular exercises under the supervision of a qualified physiotherapist, topped up with a daily home exercise regime.
When choosing a surgeon it is best to go for one who performs a large number of operations especially both types to give you the best choice for your condition.
Patients can check the surgeons profile on the National Joint Registry website which will give their results and they can compare that with the national average. It is worth asking about their revision rate. If it is high this may not be a bad sign. It may be that they are revising failed operations done by other surgeons.
Most surgeons will be putting in at least 150 new knees per year.
Awake or Asleep?
If the patient is anxious or the surgery complicated then asleep is best.
The advantage of awake is that the surgery is performed with a spinal anaesthetic. This gives the patient less pain in the early recovery phase. It is also better if you are prone to chest infections or blood clots. It also means that you do not have to recover from the general anaesthetic which in older people is a huge advantage.
Exercises before the operation
To help with a speedy recovery after surgery it is best to see a physiotherapist before surgery.
You will be shown exercises to strengthen the Quadriceps (thigh muscles) and all the muscles in the Hip which enable walking without a limp.
Ideally these should be done 4-6 weeks pre operatively.
See strengthening exercises for the knee
Exercising in water at this time may be less painful and a very good option.
Knee- Early Hydrotherapy exercises
You will probably also see an OT who will assess your needs for aids back home such as chair raisers.


The Operation
The worn ends of the thigh and shin bone including worn cartilage are removed and replaced with Titanium or cobalt chrome components
The incision will be down the front of the knee and will be around 10 inches.
Types of replacement
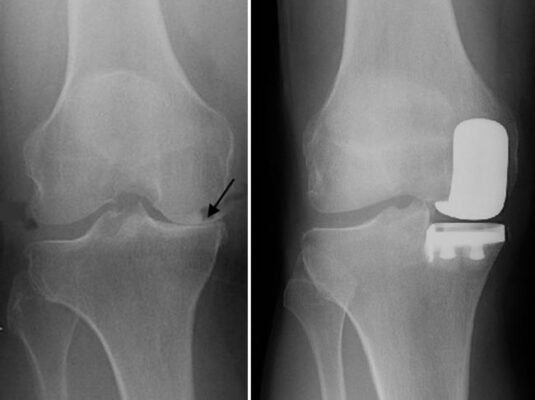
Partial (PKR)
Is most suitable for those with arthritis affecting one side of the knee and younger patients that have intact ligaments. The type of implant needs support from existing tissue.
This operation is less invasive than a total knee replacement and with less bone removed recovery is quicker. It is common with this operation to be off crutches in 2 weeks and walking normally in 4 weeks.
A recent study found that at least 50% of patients needing a replacement would be suitable for this type of operation rather than the full knee replacement. Currently only about 20% of patients receive them. These are usually the more active, younger and slimmer patients.
About 10% of patients will need another operation after 10 years
Total Knee (TKR)
This is the most common type and involves replacing joint surfaces of both the thigh bone and shin and inserting a plastic spacer in between to act like cartilage.
The most common method of securing the implant is by cementing this in to the bone.
Some implants retain the PCL (posterior cruciate ligament) which makes the knee feel more normal. This is obviously only suitable if the patients ligaments are strong enough.
It seems from research that the outcomes for leaving or removing the PCL makes little difference to the function but does add stability.
In some cases the surgeon may also replace the undersurface of the kneecap. There is an even divide amongst doctors as to whether this is a good thing to do.
After the operation
You will spend some time in recovery where you will be given fluids and painkillers. You may receive a PCA, which is a patient activated painkiller when you press a button if you need painkiller. This will go straight into your vein.
You may find you have an oxygen mask on or oxygen administered via tubes directly in to your nostrils.
If you have lost a lot of blood you may need a transfusion but normally this is not needed.
After a few days the drip with fluids and the oxygen will be removed.
Pain control will continue and you will need to keep this under control as best as you can so that you can start to exercise the knee.
The speed of recovery depends on your age, general health and general strength and mobility.
The hospital, generally, try and get you walking within 12-18 hours and home by 4 days. The physiotherapist will come and help you move and will supply and instruct you in the use of either a walking frame or crutches. They will also instruct you on stairs and how to tackle these with crutches.
Once you are safe walking alone, the wound looks healthy and there are no other medical problems you will be able to leave hospital.
The OT may come and check that you are able to dress and shower safely and will see if you need any aids at home.
If you have stitches or clips that need removal these can be done by your GP or by returning to the hospital.
Generally you return after 6 weeks for a check up
After leaving Hospital
Your physiotherapist will give you a list of the exercises to perform regularly.
It will be normal for the knee to feel stiff. It is important to do all the exercises regularly.
If the stiffness does not improve by the 6 week mark it may be necessary to manipulate it under anaesthetic.
Pain– You will have a level of pain for several months although this will gradually decrease. You may need to continue taking painkillers at night for some while so you get some sleep
Swelling– this is very common around the feet and ankles after the operation and can last a few months. You will be wearing anti embolism stocking initially, which helps with swelling and are designed to help prevent DVT (deep vein thrombosis). You will also be encouraged to move the feet up and down as much as possible when sitting or lying to encourage the circulation. Once you are walking regularly this also helps the circulation to improve.
The knee itself will also be swollen and applying ice regularly can help with pain and reduce the swelling.
Ice should be put on or around the knee for 10 minutes then allow 20 minutes rest before it is reapplied. This should be wrapped in a wet tea towel or in a plastic bag to avoid ice burns.


FAQ
When can I return to work?
This will depend on the type of work. If you sit at a desk you will probably be able to return after 6-8 weeks. If your job is more manual then you may not be able to for 10-12 weeks.
When do I feel normal again?
It will be some weeks before you recover from the operation and start to feel all the benefits of your new joint.
If you keep up the exercises with the help of regular painkillers you will make good progress. Gradually you will regain the strength in your thigh muscles and will be able to walk easier.
Try to avoid jarring and twisting activities for at least 6 weeks.
You should avoid having a bath until the wound is fully healed and you are sure that you are strong enough to get out. However, you can take a shower once the wound is dry.
Walking
Initially you will walk with crutches. Once you have sufficient strength and balance you can discard first one crutch and then go down to a walking stick. By 6 weeks you should be strong enough to walk with no aids. The time it takes depends on your age, mobility, and the type of operation you had.
When you walk try and walk without a limp. Take the same size strides with each leg and as you push off try and extend the knee.
Sitting and Kneeling
Initially try not to sit with your legs crossed as this increases the chance of blood clots.
Kneeling may never be totally comfortable again but will become easier after several months. Although uncomfortable it does not do you any harm.
Sleeping
There is no special sleeping position after knee surgery. You should avoid putting a pillow under your knees when on your back as this prevents the knee from fully extending.
However if you prefer to sleep on your side you can put a pillow between your knees in this position.
Sleeping for the first few weeks can be disturbed due to pain at night.
Driving
You will be able to drive a car again when you can safely do an emergency stop.
The normal time is about 6 weeks for a full knee replacement and 3 weeks for a partial.
If you have an automatic car and you have the left leg operated you may be able to return to driving earlier as long as you are not affected but any of the tablets you are taking.
Sport
Exercise and Sport are recommended after the operation. It is very important to do specific exercises to strengthen the thigh to help stabilise your new knee.
Bicycling is a very good exercise to build up your knee and cross trainer is also a good exercise.
You will be able to return to your normal recreational sports such as Golf, tennis (preferably doubles) and skiing.
Golf can start at 8-12 weeks with chipping and putting. Avoid the driving range for 3 months as this puts a lot of strain on the knee.
It is best to avoid contact sports as this may weaken the cement.


Complications
About 1 in 20 may have a minor complication following surgery but generally knee replacements are problem free.
Possible complications are
1. Wound Infection
Like any procedure where there is an incision there is a chance if infection. Generally this can be treated with antibiotics. If the knee becomes red, more painful and possibly a pus discharge on top of possibly a high fever you should call the orthopaedic team to have your wound checked.
2. Blood clots
You can get a deep vein thrombosis DVT. This is a clot, which forms in the deep veins of the leg. The symptoms are usually pain and an increase in swelling. The risk can be reduced with wearing the special stockings, having Heparin injections and regularly pumping your calf muscles by moving your feet up and down. It is also important to avoid crossing your legs.
3. Pulmonary Embolism
Occasional a clot can travel to the lungs and causes a pulmonary embolism. The symptoms of this are breathlessness and pain in the chest.
If you have this symptom seek urgent medical attention. You will be put on clot busting drugs and blood thinning medication.
4. In rare cases there is damage to nerves, ligaments and blood vessels
5. Bleeding and wound Haematoma
The bleeding should stop after about 2 days post surgery. Occasionally the blood collects and builds up under the skin. This usually resolves itself but occasionally requires intervention by the surgeon
6. Pain
A few people have ongoing pain after the normal period expected.
These people may then need to be referred to a pain clinic
7. Stiffness
it is usual to be stiff for the first few months. This usually feels better after the exercise regime. In rare cases this stiffness does not resolve and a manipulation under anaesthetic is performed.
Travelling/Flying
Try and avoid flying for at least 6 weeks after surgery to avoid the danger of blood clots. Flying Long haul is not advised for 3 months after surgery.
Everything you wanted to ask the knee surgeon and forgot!!
An interview with Mr Edward Crawfurd FRCS
Click here to watch the film