When to seek immediate medical attention
Any change in pain, altered sensation, skin colour, or redness and swelling which may be caused by an infection or the cast may be too tight or loose.
You should not drive, carry heavy objects or participate in sport whilst the cast is on.
After removal of the splint
When the cast comes off you will usually be given a removable wrist splint,
From here on the next phase of rehab begins.
Your wrist will feel stiff and weak and the muscle bulk of the forearm will have wasted.
It is important to work on regaining a full range of movement in all planes with especial attention being paid to ensuring a good grip.
Best results are achieved by exercising the wrist little and often with periods of rest in the splint, some pain and discomfort is to be expected during this phase of recovery. As movement and strength returns the time in the splint is reduced until you have weaned yourself off its use, this can be another 6 weeks.
You may not feel that you are fully recovered for up to 6 months following the initial injury but you should feel progress is being made steadily throughout this period.
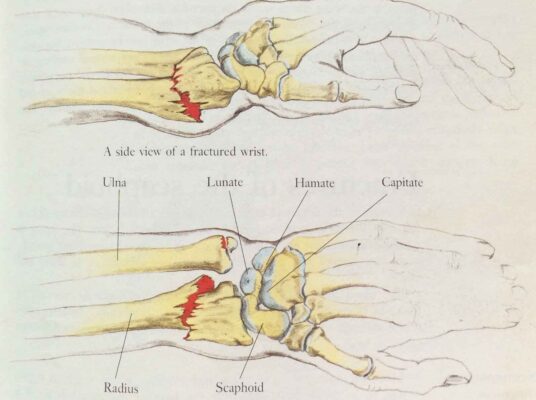
Complications associated with this injury can include an ulnar styloid fracture
More serious complications that can arise with a more complex scenario include Intra articular involvement of the articular surfaces, which will require surgery via open reduction and internal fixation (ORIF), using wires, plate, screws or rods to realign the fracture.
Other complications can cause median nerve damage, post traumatic carpal tunnel syndrome, reflex sympathetic dystrophy, tear or rupture of the extensor pollicis longus tendon, and ligament damage.